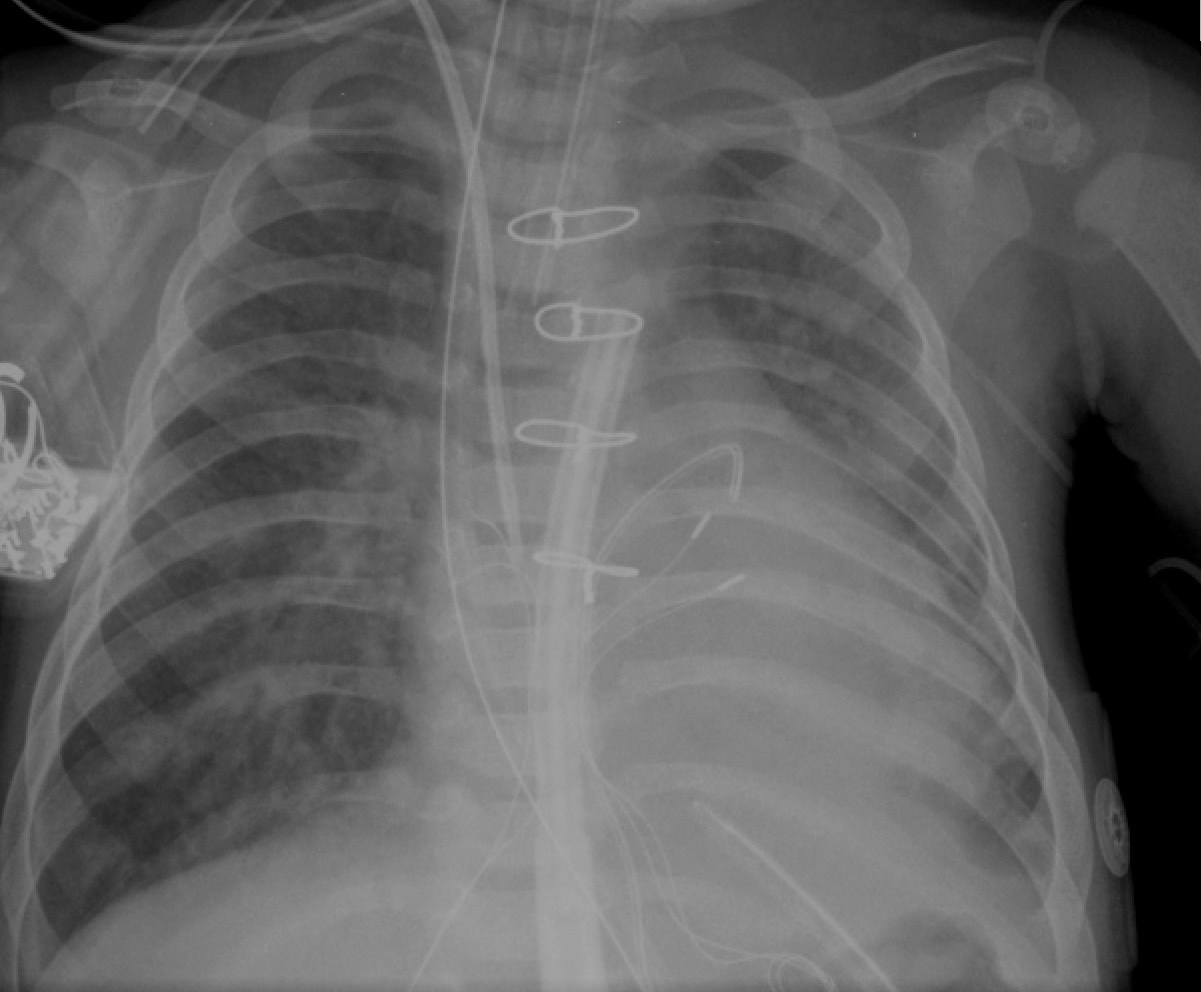
PA and Lateral views of venous and arterial catheter are provided.
Question 1: Trace the course of venous catheter. What diagnosis does this catheter-course leads you to?
Answer: Venous catheter-course: IVC - RA - PFO - LA - Left AV valve - morphologic RV (mRV) on the left side - Pulmonary valve - MPA - RPA. Diagnosis: Transposition of great arteries (L-TGA - Aortic valve is anterior in lateral view and to the left of the pulmonary valve in PA view)
Questoin 2: Trace the arterial catehter. Which side if the aortic arch?
Answer: Arterial catheter-course: Descending aorta - Aortic arch - Ascending aorta. Lateral view shows that the aorta is anterior. Aortic arch is left sided. Trachea is deviated towards the right. Apparent appearance of descending aorta on the right side of spine is misleading. Note the typical location of the ascending aorta in L-TGA. This causes a unique, fullness in the left, superior mediastinum in CXR.



































{kind=link}
{kind=link}
{kind=link}